Monday Feb 23, 2026
Monday Feb 23, 2026
Friday, 18 November 2016 00:00 - - {{hitsCtrl.values.hits}}
 By Priyanka Jayawardena
By Priyanka Jayawardena
Sri Lanka provides free healthcare for all citizens, which has been a national priority for decades. With a wide network of healthcare services, the country’s public sector healthcare delivery system accounts for almost all preventive care and most in-patient care.
While the public healthcare delivery system is remarkably successful in providing a universal service, there are certain limitations in the system, especially in the provision of curative care such as drug shortages, limited out-patient care services (obtaining appointments before 12 noon, longer waiting times, etc.), and limited access to specialist care. These reasons have created a demand for private sector healthcare services. The private sector also plays an important role to fill this gap, but it results in out-of-pocket (OOP) expenditure for healthcare.
Despite the free healthcare services in the public sector, which include doctors’ fees, medicine costs, laboratory tests, and hospital charges, households still spend a considerable amount of money on health. For example, according to the Household Income and Expenditure Survey (HIES) 2012/13, on average, a household spends around Rs. 1,564 per month on health, which accounts for 4% of the household budget. This health OOP expenditure may be too much for some people and raises concern on the factors that drive these costs in the context of the country’s free healthcare policy. Given this backdrop, the article explores some policy options of the country’s health sector.
What are the driving costs of health OOP?
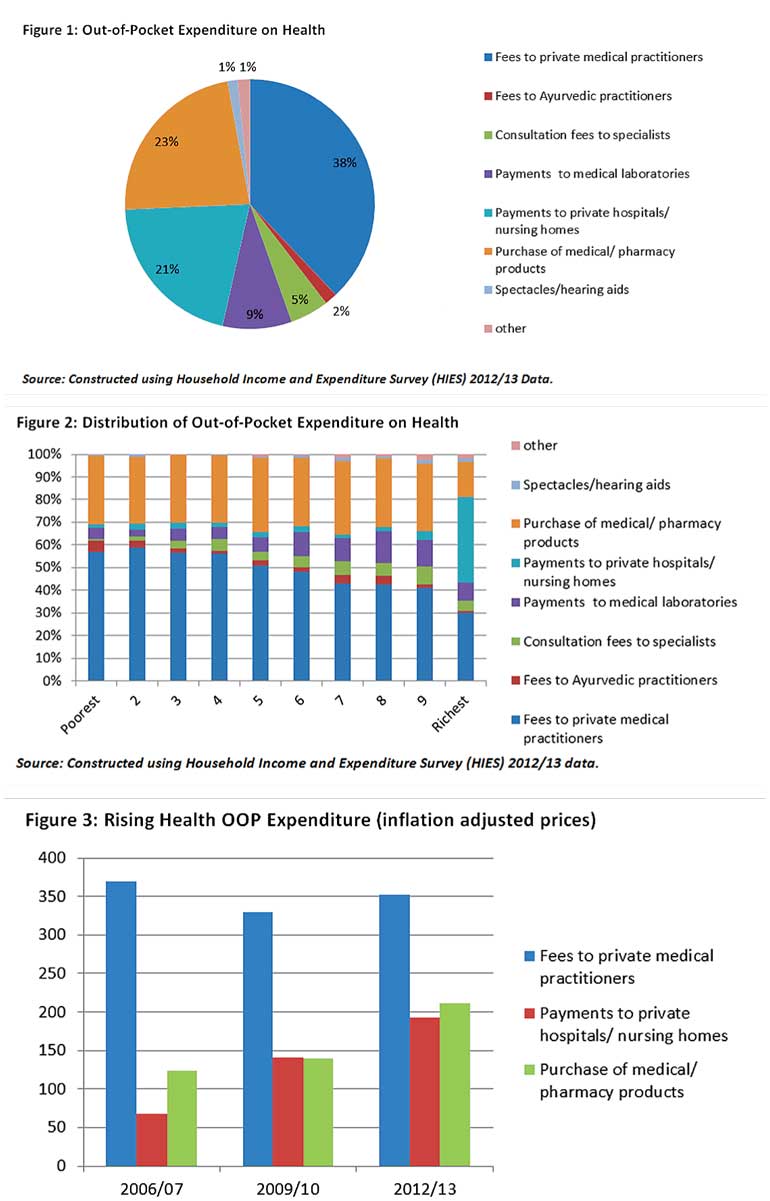
Most of the health OOP expenditures are on private doctors’ fees. The country’s health system allows anyone to directly go to a government or a private dispensary/hospital, or consult a specialist in a private hospital. Despite free healthcare services, households spend around 38% of the health OOP expenditure on doctors’ fees (see Figure 1). However, specialists’ care accounts for only 5% of the households’ health spending, which implies that in most cases people need the doctor’s basic service, that is available free of charge in all government hospitals.
On the other hand, a majority of the private practitioners serve at public sector hospitals during the day. Then, why do people opt for private consultations? The main reason could be the opportunity cost, as public sector OPD service hours are limited, if they go to a government hospital, they have to take a day off from their workplaces. Therefore, when a family member falls ill, the breadwinner generally prefers to go to a private medical doctor so they do not have to compromise their day-wage. Another reason for seeking a private medical practitioner is the shortage of medicine in government hospitals.
The second largest driver of OOP healthcare costs is medicine. Households spend around one-fourth of their OOP health spending on medicine, however, many families cannot afford the high rates, especially those undergoing treatment for chronic diseases. Yet, they end up spending a high price on medicine. While one reason for this is seeking healthcare from private practitioners, the other pertinent reason is the prevailing drug shortages in government hospitals.
Due to drug shortages, doctors prescribe medicine to buy from outside and people have to bear the cost. As a result, people opt to go for private practitioners, as they anyway have to bear the medicine cost.
The third highest health OOP expenditure is on hospital charges, which accounts for 21% of health OOP expenditure. However, this cost mostly involves the richest decile people (see Figure 2).
Burden of health OOP on poor
It is clear that the private doctor fees and the medicine costs are the main drivers of health costs for lower income groups (see Figure 2). For example, 57% of the health OOP expenses, of the lowest decile households are for doctors’ fees followed by 30% of OOP health expenses for medicines. The households that report non-zero private doctor fees spend around Rs. 1,500 per month for doctors while households who reported non-zero medicine cost, spend around Rs. 1,196 per month for medicine. Are these costs affordable to the poor? More importantly, how have these costs changed over time?
Figure 3 depicts that the inflation-adjusted prices of main health OOP expenditure items medical and pharmaceutical products and hospital fees have increased over the period while private doctor fees remain high but have not varied much during the period. The high private doctor fees and increasing medicine prices may pose a threat to household welfare, especially for families with patients who need long-term care for Non-Communicable Diseases (NCDs) such as heart diseases, diabetes, etc.
Furthermore, with the growing ageing population and increasing burden of NCDs (15% of the total population receive treatment for any acute illness), which requires a patient to intake medicine for a long period, medical investigations, frequent visits to doctors, will also result in an increase in OOP expenditure in the future.
With the aim of controlling the medicine prices, the present government has taken some initiatives to regulate the prices of medical drugs. The much-debated National Medicinal Drugs Regulatory Authority Bill was ratified in March 2015. Recently the Government introduced a controlled price for 48 essential pharmaceutical drugs based on the new pricing mechanism – Maximum Retail Price (MRP) formula. However, there are many challenges in its implementation such as the cost of imported dugs, availability of good quality drugs etc.
Addressing critical concerns
The burden of health OOP expenditure definitely affects household welfare. With the rising ageing population and the increasing demand for long-term care, the household welfare can be further burdened. There should be certain price regulations on most essential healthcare services such as private medical practitioner fees, prices of essential drugs, etc. It is also important that the Government should take urgent action to smoothen the implementation of the controlled price on essential drugs. With the aim of increasing accountability of private doctor consultations, the Government could also consider introducing a Government authorised receipt system.
In addition, it is a necessity to improve access to free healthcare services. The Government should consider expanding out-patient services especially in rural areas giving flexibility for income earners of the family. In addition, it is necessary to take measures to solve the drug shortages in government hospitals.
(Priyanka Jayawardena is a Research Economist at the Institute of Policy Studies of Sri Lanka (IPS). To view the article online and comment, visit the IPS blog ‘Talking Economics’ – www.ips.lk/talkingeconomics).


