Thursday Feb 19, 2026
Thursday Feb 19, 2026
Wednesday, 28 September 2016 00:01 - - {{hitsCtrl.values.hits}}

By Dr. Srikanth Srinivasan
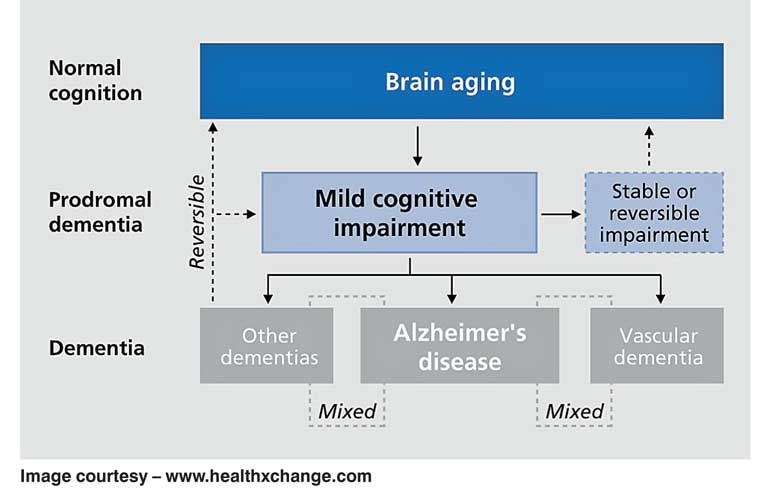
Dementia is a brain condition that causes memory loss commonly but can also result in speech disturbances, way finding difficulties and difficulty with complex multi-step activities. These disturbances occur in clear consciousness and are sufficiently severe to impair the day to day functioning of the affected individual. A significant proportion of patients with dementia also develops behavioural and psychological symptoms such as depression, hallucinations and delusions, agitation and sleep problems.
Mild Cognitive Impairment (MCI) is the intermediate stage between normal ageing and dementia. In MCI, patients exhibit memory and other cognitive impairment but function normally to a great extent. However in dementia the cognitive deficits interfere with day to day functioning.
Mild Cognitive Impairment and dementia are primarily prevalent among the elderly. 8-10 % of the world’s elderly population (over the age of 65 years) suffer from dementia due to various causes. In Sri Lanka 3-4 % of the elderly over the age of 65 years have dementia. Though it is a common problem in the geriatric age group, it is by no means restricted to the elderly.
In the author’s own sample of about 600 patients with cognitive impairment, about 20% (one fifth) of patients are below the age of 65 years. It is also estimated that 15-20% of the population over the age of 65 years may experience MCI. In other words, for every person with dementia in the community there are two or three persons with MCI.
There are modifiable and unmodifiable risk factors in dementia. The unmodifiable risk factors are ageing and family history. The modifiable risk factors are low education, serious head injury, vascular risk factors such as hypertension, diabetes and high cholesterol levels, depression in middle or late life and excessive alcohol consumption. The single most protective factor against dementia is high early life education.
The commonest cause of dementia the world over is Alzheimer’s Disease. This is a neurodegenerative disorder that causes death and dysfunction of neurons in the brain especially in the regions responsible for memory. The harmful protein called amyloid protein is deposited in the neurons [brain cells] and is the cause of nerve cell death and symptoms of Alzheimer’s disease.
Typically, AD is a disease of gradual onset and progression and causes impairment of recent memory first. As the illness advances, word finding difficulties, way-finding difficulties and difficulties with complex multistep activities like cooking, emerge. In the more advanced stages of AD, psychiatric problems such as depression, psychosis, agitation and sleep problems emerge. AD is an inexorably progressive brain condition that ultimately results in the death of the individual after about 8 to 10 years. Very rarely AD can first present with symptoms other than memory loss.
Vascular dementia is the next commonest cause of dementia and cognitive impairment in the elderly. There are many different subtypes of vascular dementia but the commonest one is where small silent strokes accumulate in the deep parts of the brain and result in cognitive impairment. These small silent strokes also cause walking difficulties and urinary incontinence.
The next most common of this kind is Parkinsonian dementia. This primarily result in disorders of motor skills such as tremors, slowness, rigidity and stiffness of hands and legs with falls and gait disturbances. Many of these patients also have prominent hallucinations and false/suspicious beliefs [delusions]. Some of these patients also have dream enactment behaviour which is a distinctive symptom in this group of dementias.
Primarily affecting middle aged people is the group of dementias called Frontotemporal dementia. Changes in personality and behaviour are the first and most prominent alterations in these patients. Patients become either withdrawn or uninhibited, develop strange routines or habits, change eating behaviour and lose empathy and compassion. Subsequently as the illness advances other symptoms like forgetfulness or speech disturbances can develop.
The next important group of dementias is the Reversible dementias group which includes conditions like Normal Pressure Hydrocephalus, Brain tumours, Subdural haemorrhage and various metabolic disorders like thyroid deficiency, vitamin B12 deficiency, brain infections like HIV/AIDS and neurosyphilis.
Diagnosis of MCI and dementia – When a patient presents with a complaint of memory loss a detailed history is taken from the caregivers. Then a memory test is done on the patient; usually a brief screening test but rarely more detailed testing called neuropsychological assessment. A physical examination is also conducted and then tests ordered to find out the cause of dementias. These typically include a brain scan such as CT or MRI scans, blood tests and rarely lumbar puncture and spinal fluid examination. Once the cause of the dementia is determined, appropriate treatment is started.
Treatment of MCI and dementia – For most degenerative or vascular dementias, no treatment currently exist to reverse the symptoms. The best effect of currently available medications is to slow down the progression of brain degeneration. Vascular dementia offers a study in contrast. It can actually be prevented by treating risk factors for stroke such as high blood pressure, diabetes and high cholesterol levels. On the other side behavioural and psychological symptoms of dementia which are a considerable source of stress for family caregivers can be controlled to a great extent by using antidepressants, antipsychotics and sleep promoting agents. In carefully selected cases of Normal Pressure Hydrocephalus neurosurgery in the form of ventriculoperitoneal shunting offers a promise for cure. It is important to identify MCI early because it may offer real possibilities that the individual can actually be prevented from developing dementia.
Prevention of MCI and dementia – The greatest hope in the fight against dementia at present is to prevent or delay the onset of symptoms. Scientific research has started to show us the way in the right direction. Some of the measures that have been shown to be valid in distancing dementia are as follows: Mentally stimulating hobbies or leisure activities such as crossword puzzles, sudoku or other board games like chess or bridge; learning a new language; strict control of high blood pressure, diabetes and high cholesterol levels; regular physical exercise; quitting smoking and moderating alcohol consumption; consuming a diet rich in olive oil, vegetables and fruits, oily cold water fish and curtailing the consumption of red meat – the so-called ‘Mediterranean Diet’; treatment of depression if present and identification and treatment of sleep problems including insomnia and sleep apnea.
(The writer is Consultant Neurologist, Lanka Hospitals PLC.)


